What Is a Kidney Transplant?
A kidney transplant is when a healthy kidney from a donor is placed into someone whose own kidneys no longer work. It’s not a cure, but it’s the best treatment for end-stage renal disease (ESRD). People who get a transplant live longer, feel better, and don’t need to spend hours hooked up to a dialysis machine three times a week. The first successful transplant happened in 1954 between identical twins, and since then, over 800,000 people worldwide have received one.
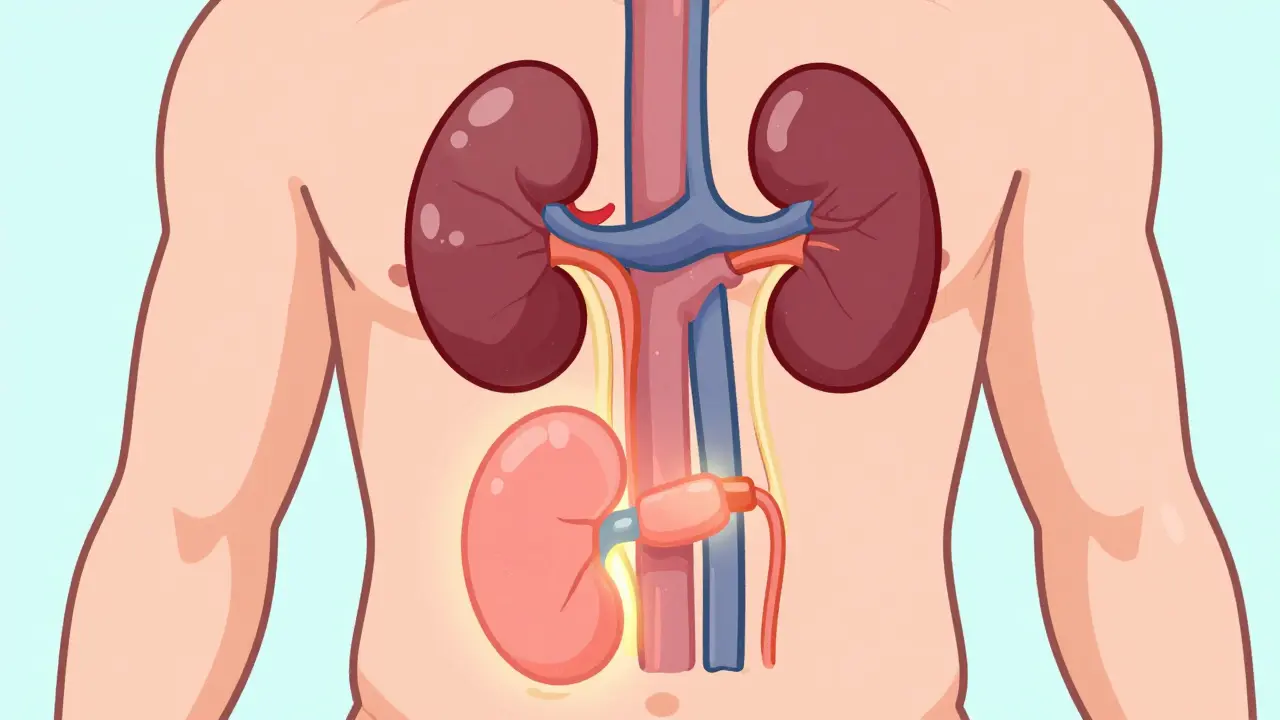
Unlike other organ transplants, your original kidneys are usually left in place. The new kidney is placed in your lower belly, and its blood vessels and ureter are connected to your own. You don’t need to remove the old ones unless they’re causing infections, high blood pressure, or pain.
Who Can Get a Kidney Transplant?
You don’t need to be perfect to qualify-but you do need to be well enough to survive the surgery and stick to a strict lifelong care plan. Most transplant centers require you to have end-stage renal disease, meaning your kidneys are working at 15% or less of normal capacity. This is measured by your glomerular filtration rate (GFR), which should be 20 mL/min or lower. Some centers will consider you even if your GFR is up to 25 mL/min if your kidney function is dropping fast or you already have a living donor lined up.
Age isn’t a hard cutoff. While some centers may hesitate with patients over 75, others evaluate older adults based on overall health, not just age. What matters more is whether your heart, lungs, and other organs can handle the surgery and recovery.
What Disqualifies Someone?
Not everyone who needs a transplant can get one. There are clear medical reasons that make the risk too high. These are called absolute contraindications:
- Active cancer that hasn’t been treated or is likely to come back
- Untreated or uncontrolled infections like tuberculosis or hepatitis B with active virus
- Severe mental illness that makes it impossible to take daily medications
- Ongoing drug or alcohol abuse
- HIV with a CD4 count below 200 or detectable viral load
Some conditions aren’t automatic disqualifiers but make the process harder. For example, a BMI over 35 is considered risky, and over 45 usually blocks approval. Obesity increases the chance of surgical complications by 35% and raises the risk of the new kidney failing by 20%. Many centers require patients to lose weight before being listed.
Heart and lung health are also critical. If you have severe pulmonary hypertension-where pressure in your lung arteries is over 70 mm Hg-you won’t qualify. If you’re on oxygen full-time because of COPD or another lung disease, you’re typically not a candidate. Your heart needs to be strong too: an ejection fraction below 35-40% usually means you’re too high-risk.
The Evaluation Process
Getting approved for a transplant isn’t just about your kidneys. It’s a full-body checkup that takes weeks or even months. You’ll go through:
- Blood tests for infections, tissue type, and antibodies
- Cancer screenings like colonoscopies and skin checks
- Heart tests: echocardiogram, stress test, sometimes a cardiac catheter
- Lung function tests and chest X-rays
- Psychological evaluation to assess your ability to manage lifelong care
- Social work review to confirm you have support at home
Many centers now use frailty assessments, especially for patients over 60. These look at things like grip strength, walking speed, weight loss, and how tired you feel. If you’re frail, your chances of surviving surgery drop. That’s why some centers require you to build up strength before being listed.
You’ll also need a care partner-a family member or close friend who will help you take your meds, drive you to appointments, and call the doctor if something feels wrong. This isn’t optional. Studies show transplant recipients without strong support are twice as likely to lose their new kidney.
What Happens During Surgery?
The surgery itself takes about 3 to 4 hours. You’ll be under general anesthesia. The surgeon places the new kidney in your lower abdomen, connects its main artery and vein to your blood vessels, and attaches the ureter to your bladder. The whole thing is done without opening your old kidney area.
Most of the time, the new kidney starts working right away. You’ll see urine flowing into your bladder within minutes. But in about 20% of cases-especially with kidneys from deceased donors-the organ takes a few days to start working. That’s called delayed graft function. You might need dialysis for a short time until the kidney kicks in.
Recovery takes about 4 to 6 weeks. You’ll be in the hospital for 3 to 7 days, depending on how things go. Pain is managed with medication, and most people are walking the day after surgery. You won’t be able to lift anything heavy for at least 6 weeks.
Life After Transplant: The Lifelong Commitment
Getting a new kidney isn’t the end-it’s the beginning of a new routine. You’ll need to take immunosuppressant drugs every single day, for the rest of your life. These drugs stop your immune system from attacking the new kidney. The standard combo includes:
- A calcineurin inhibitor (tacrolimus or cyclosporine)
- An antiproliferative drug (mycophenolate or azathioprine)
- A steroid (prednisone)
Some people get extra drugs right after surgery (induction therapy) to give the new kidney a better start.
These drugs save your kidney-but they come with side effects. You might gain weight, get higher blood sugar, have high blood pressure, or face a slightly increased risk of infections and certain cancers. That’s why regular checkups are non-negotiable.
For the first month, you’ll go in weekly. Then monthly for the next 3 to 6 months. After that, you’ll see your transplant team every 3 months, and once a year for life. Blood tests check your kidney function, drug levels, and signs of rejection. Even if you feel fine, skipping a visit can cost you your transplant.
Success Rates and What to Expect
Kidney transplants have high success rates. In the first year, 95% of living donor transplants are still working. For deceased donor kidneys, it’s 92%. At five years, about 85% of living donor kidneys are still going strong. For deceased donor kidneys, that number drops to 78%.
That means if you get a transplant, you’re far more likely to live longer than if you stay on dialysis. Five-year survival on dialysis is around 50%. With a transplant, it’s about 85%.
Living donor transplants are better for a few reasons. The kidney works faster, lasts longer, and you can schedule the surgery before you get too sick. Deceased donor kidneys often come from people who died unexpectedly, so they’re not always in perfect condition. The Kidney Donor Profile Index (KDPI) helps match kidneys with the best expected lifespan to patients who need them most.
What About New Advances?
Science is moving fast. Researchers are testing ways to help the body accept a new kidney without lifelong drugs. Some trials are using special cell therapies or immune system training to create “tolerance.” If this works, it could change everything.
Organ preservation has improved too. New machines can keep kidneys alive outside the body longer and even repair damaged ones before transplant. This means more kidneys from older donors or those with minor health issues can now be used safely.
And yes-people with HIV and hepatitis C can now get transplants, thanks to better antiviral drugs. In the past, these conditions were automatic disqualifiers. Now, they’re manageable conditions.
What If the Transplant Fails?
It happens. About 1 in 5 transplants fail within 5 years. Reasons include rejection, side effects from drugs, or the kidney simply wearing out. If it fails, you go back to dialysis. You can be relisted for another transplant, and many people get a second-or even third-kidney.
Some people choose to stay on dialysis instead of going back on the list. That’s a personal decision. But if you’re healthy enough, a second transplant often gives you another 10-15 years of good life.
Final Thoughts
A kidney transplant isn’t a quick fix. It’s a major surgery followed by a lifelong commitment to health. But for most people, it’s the best chance to live a full, active life again. You can travel, work, exercise, and spend time with family without being tied to a machine.
If you’re considering a transplant, talk to your nephrologist early. Get evaluated. Build your support system. Take care of your heart and weight. The sooner you start, the better your odds.
Can you live a normal life after a kidney transplant?
Yes, most people return to normal activities within a few months. You can work, travel, exercise, and even have children. But you must take your anti-rejection meds every day, attend all follow-ups, and avoid infections. Many people say they feel better after a transplant than they did before they got sick.
How long do kidney transplants last?
On average, a kidney from a living donor lasts 15-20 years. A kidney from a deceased donor lasts 10-15 years. Some last longer-over 30 years in rare cases. But even if it fails, you can go back on dialysis and get another transplant.
Can anyone be a living kidney donor?
Most healthy adults between 18 and 70 can donate. They need to be blood type compatible, have normal kidney function, and pass medical and psychological screening. Donors don’t need to be related. Many people donate to friends, coworkers, or even strangers through paired exchange programs.
Do you need to be on dialysis before getting a transplant?
Not always. Many people get transplants before they start dialysis-this is called preemptive transplantation. It’s often better because you avoid the physical toll of dialysis. But most centers require your kidney function to be very low (GFR under 20) and your condition to be worsening.
What are the biggest risks after a transplant?
The biggest risks are rejection, infection, and side effects from immunosuppressants. Rejection can happen anytime, even years later. Infections are more common because your immune system is suppressed. Long-term, you have a higher risk of skin cancer, lymphoma, and metabolic issues like diabetes and high blood pressure. Regular checkups catch these early.
Can you drink alcohol after a kidney transplant?
Moderate alcohol is usually okay-like one drink a day. But heavy drinking harms your liver and can interact with your medications. Some transplant centers recommend avoiding alcohol entirely, especially in the first year. Always check with your transplant team.
How much does a kidney transplant cost?
In the U.S., the average cost is $400,000-$500,000 for the surgery and first year of care. Insurance, including Medicare, usually covers most of it. In the UK, the NHS covers the full cost. Ongoing medication costs around $2,000-$5,000 per year, depending on the drugs. Financial counselors at transplant centers help patients navigate costs and assistance programs.
Comments
Stewart Smith
I used to think dialysis was just a waiting room for death. Then I saw my uncle get a transplant after 4 years on it. He started hiking again. I cried watching him carry his grandkid on his shoulders. No meds are perfect, but this? This is life.
December 30, 2025 at 21:07
Aaron Bales
GFR under 20 is the standard threshold. But if you’re declining fast and have a living donor, some centers will list you at 25. Don’t wait until you’re desperate. Get evaluated early.
December 31, 2025 at 16:09
John Chapman
Living donor = better outcomes. Period. 🙌 My sister gave me her kidney. I didn’t just get a new organ-I got a second chance at being present for my kids. No regrets. Zero.
January 1, 2026 at 14:12
Retha Dungga
Life after transplant is like being reborn but with a monthly bill from the pharmacy 🤕💊 but hey at least you can eat pizza without asking permission from a machine 🍕
January 2, 2026 at 15:35
Urvi Patel
Why do Americans treat transplants like some miracle when we have entire nations where dialysis is a luxury? You talk about 95% success rates like its a tech upgrade not a privilege reserved for the insured
January 4, 2026 at 12:21
Darren Pearson
The notion that age is not a contraindication is statistically misleading. While individual cases exist, the mortality risk for patients over 75 undergoing transplant exceeds 25% within the first year. The data does not support broad optimism. One must consider not merely survival, but quality-adjusted life years.
January 5, 2026 at 14:05
Joy Nickles
I read this whole thing and I’m like… why is no one talking about the fact that the immunosuppressants make you gain like 40 pounds?? I mean, I know it’s necessary but like… I look like a balloon with a kidney inside?? 😭😭😭 and the acne?? the moon face?? the diabetes?? I didn’t sign up for this.
January 6, 2026 at 12:14
Kayla Kliphardt
I’m curious-how many people are turned down because they can’t afford the follow-up meds, even if they qualify for the surgery? The article mentions costs, but doesn’t address the real barrier.
January 7, 2026 at 04:51
Jenny Salmingo
My cousin got a kidney from a stranger in another state. She didn’t know her name. But she sends her a card every year. Just says ‘thank you for letting me breathe.’ That’s more than medicine. That’s love.
January 8, 2026 at 23:52
anggit marga
You Americans act like transplant is some great achievement but in Nigeria we have people who die waiting because hospitals don’t have the basic tools to even check for infection. Your success rates mean nothing when the system is rigged for the rich. This isn’t science-it’s capitalism with a stethoscope
January 10, 2026 at 03:13