Polycystic Ovary Syndrome, or PCOS, isn’t just about irregular periods or acne. For millions of women, it’s a persistent hormonal puzzle that affects everything from fertility to long-term health. If you’ve been trying to get pregnant and nothing seems to work, or if you’ve been told your cycles are "normal" but you still don’t ovulate, you’re not alone. About 5-10% of women of reproductive age have PCOS, and many don’t get diagnosed until they hit a wall with fertility. The truth? It’s not a mystery-it’s a measurable imbalance, and we know exactly how to fix it.
What’s Really Going On Inside?
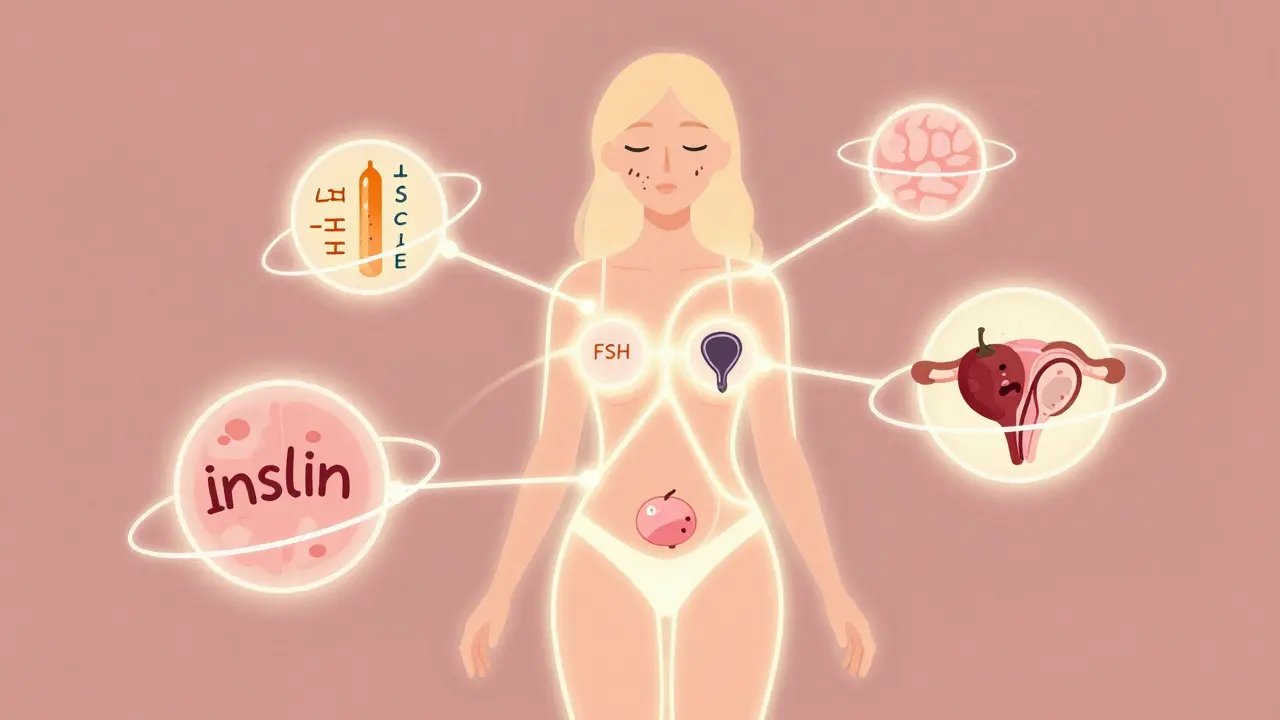
PCOS isn’t caused by one thing. It’s a chain reaction. At its core, it’s about hormones going off track-especially insulin, testosterone, and LH (luteinizing hormone). Most women with PCOS have insulin resistance, even if they’re not overweight. That means their body doesn’t respond well to insulin, so it makes more of it. High insulin levels tell the ovaries to crank out testosterone, which is the main reason for symptoms like facial hair, acne, and thinning scalp hair.At the same time, the brain’s signals get mixed up. LH, which should rise mid-cycle to trigger ovulation, stays too high. FSH, which helps eggs mature, stays low or normal. The result? Eggs don’t mature properly. They just sit in the ovaries like unripe fruit, forming the "cysts" you hear about on ultrasounds. But here’s the catch: you don’t need cysts to have PCOS. The diagnosis is based on two out of three things: irregular ovulation, signs of high androgens (like hirsutism or blood tests), and polycystic ovaries on scan.
Progesterone? It’s often missing. Without ovulation, there’s no corpus luteum to make progesterone. That’s why periods become erratic-or vanish. And because estrogen is still there without progesterone to balance it, the lining of the uterus keeps building up. That’s why women with untreated PCOS have a 2-6 times higher risk of endometrial cancer. This isn’t just a fertility issue. It’s a metabolic time bomb.
Fertility Treatment: What Actually Works?
If you’re trying to conceive, the good news is PCOS is one of the most treatable causes of infertility. The first step isn’t medication-it’s lifestyle. Losing just 5-10% of your body weight can restore ovulation in up to half of overweight women. That doesn’t mean starving yourself. It means moving more and eating smarter. Studies show 150 minutes of brisk walking or cycling per week, paired with a 500-750 calorie daily deficit, leads to real, lasting results. The Diabetes Prevention Program protocol, originally designed for prediabetes, works just as well for PCOS. In fact, 44% of women who were previously anovulatory started ovulating after six months of this approach.When lifestyle alone isn’t enough, doctors turn to medication. Clomiphene citrate (Clomid) has been the go-to for decades. It works by tricking the brain into thinking estrogen is low, so it pumps out more FSH to trigger ovulation. About 60-85% of women ovulate on Clomid, and 30-40% get pregnant within six cycles. But for many, it stops working. That’s where letrozole comes in.
Letrozole, originally a breast cancer drug, is now the first-line choice for many fertility specialists. In the landmark PPCOS-II trial, letrozole led to a 27.5% live birth rate compared to just 19.1% with Clomid. It’s especially effective for women with higher BMI or insulin resistance. And unlike Clomid, it doesn’t thin the uterine lining, which may explain why pregnancy rates are higher.
Metformin? It’s not a fertility drug-but it helps. It lowers insulin, which lowers testosterone. It’s not strong enough on its own to make you ovulate, but when paired with Clomid or letrozole, it can boost pregnancy rates by 30-50%. That’s especially true for women with a BMI over 35. Side effects? Nausea and diarrhea. But those usually fade if you start low and go slow-1,000 mg a day, taken with meals.
When Medication Isn’t Enough
About 20-25% of women don’t respond to oral drugs. That’s when injectable fertility medications-gonadotropins-come into play. These directly stimulate the ovaries with FSH and LH. They’re powerful. Pregnancy rates hit 15-20% per cycle. But they come with risks: a 20-30% chance of twins or triplets, and a 5-10% risk of ovarian hyperstimulation syndrome (OHSS), where the ovaries swell and leak fluid. That’s why monitoring with blood tests and ultrasounds is non-negotiable.IVF is the next step, but it’s not always the best first choice. PCOS patients often need lower doses of stimulation drugs than others-150-225 IU per day instead of 225-300 IU-because their ovaries are so sensitive. But that sensitivity also means higher OHSS risk (10-20% vs. 1-5% in non-PCOS). Still, IVF success rates for PCOS women are just as good as for other infertility causes. The key? Working with a clinic experienced in PCOS. They’ll use gentler protocols, freeze all embryos (to avoid OHSS), and transfer one at a time.
What No One Tells You
Most doctors focus on ovulation. But PCOS is more than that. Stress matters. Chronic stress raises cortisol, which throws off the whole HPO axis-the brain-ovary communication line. Sleep? Poor sleep worsens insulin resistance. Mental health? Depression and anxiety affect 30-50% of women with PCOS. Yet, only 32% of those surveyed in 2022 received any mental health screening.And then there’s the stigma. Many women say they’ve been told to just "lose weight" as if it’s a choice, not a physiological battle. A 2022 survey found 78% of women with PCOS felt judged by healthcare providers because of their weight. That’s not just unfair-it’s harmful. Weight loss helps, but it doesn’t cure PCOS. Even thin women have it. And even if you lose weight, you still need ongoing care.
That’s why integrated care is changing outcomes. Women who see an endocrinologist, a reproductive specialist, and a dietitian together have 30% higher pregnancy rates. Why? Because PCOS isn’t one problem. It’s a cluster: hormonal, metabolic, emotional, and reproductive. Treating one part without the others is like fixing one wheel on a car with three flat tires.
The Bigger Picture: Long-Term Health
PCOS doesn’t end when you get pregnant. In fact, the risks just shift. By age 40, half of all women with PCOS will develop type 2 diabetes. Their risk of heart disease is doubled. That’s why fasting glucose and lipid panels should be checked every year-no matter how young you are. Even if you’re not trying to conceive now, you need to protect your future.New tools are emerging. In 2022, the FDA approved Femaloop PCOS, a digital app that guides users through personalized diet, exercise, and sleep plans. In trials, it improved menstrual regularity by 28% in six months. AI algorithms are being trained to predict PCOS with 92% accuracy using just AMH levels, LH:FSH ratios, and ovarian volume. These aren’t sci-fi-they’re here.
The future of PCOS isn’t one-size-fits-all. It’s personalized. Some women need insulin-lowering meds. Others need stress management. Some need fertility drugs. Others need to focus on metabolic health first. The goal isn’t just pregnancy-it’s lifelong health.
Can you get pregnant with PCOS without medication?
Yes, some women do. Losing 5-10% of body weight can restore natural ovulation in up to half of overweight women with PCOS. Regular exercise, a low-glycemic diet, and better sleep can help reset hormones. But if you’ve been trying for over a year without success, it’s time to talk to a specialist. PCOS isn’t always resolved with lifestyle alone.
Is letrozole better than Clomid for PCOS?
Yes, for most women. The 2014 PPCOS-II trial showed letrozole led to higher ovulation rates (88% vs. 70%) and more live births (27.5% vs. 19.1%) than Clomid. It’s now the first-line drug recommended by major guidelines. Clomid still works, but letrozole is more effective, especially for women with higher BMI or insulin resistance.
Does metformin help you get pregnant?
Metformin alone rarely causes ovulation-it works in about 15-40% of cases. But when combined with Clomid or letrozole, it can boost pregnancy rates by 30-50%, especially in women with insulin resistance or a BMI over 35. Its main job is to lower insulin, which reduces testosterone and improves egg quality. It’s a support player, not the star.
Can PCOS be cured?
There’s no cure for PCOS. It’s a lifelong condition. But symptoms can be managed so well that many women live without noticeable issues. Ovulation can return. Periods can become regular. Fertility can be restored. The key is consistent care: diet, movement, stress management, and regular health checks. You’re not broken-you’re managing a complex hormonal system.
Why do some women with PCOS have normal weight?
Insulin resistance in PCOS isn’t tied to body weight. About 20-30% of women with PCOS are lean. Their bodies still overproduce insulin in response to carbs, even if they don’t carry extra fat. This drives excess androgen production, leading to the same symptoms: irregular cycles, acne, and infertility. Weight isn’t the cause-it’s just one factor. You can have PCOS and be thin.
Comments
Kevin Siewe
Just wanted to say this post nailed it. I’ve been living with PCOS for 8 years, and no one ever explained the insulin-testosterone link like this. It’s not about being lazy or eating too much sugar-it’s biology. I lost 12% of my body weight and started ovulating naturally. No meds. Just consistent movement and protein-heavy meals. Game changer.
March 23, 2026 at 08:32
Chris Farley
So you’re telling me the government’s sugar policies are why women can’t get pregnant? Classic left-wing narrative. You’re blaming the system instead of personal responsibility. I’ve got a cousin who ate pizza every day and had triplets. Coincidence? I think not.
March 24, 2026 at 10:49
Darlene Gomez
Thank you for writing this with so much nuance. I’m a therapist who specializes in women’s health, and I can’t tell you how many clients come in feeling broken because their doctor said, ‘Just lose weight.’ The shame is real. But the science here? It’s empowering. PCOS isn’t a failure-it’s a signal. Your body’s trying to tell you something. Listening is the first step to healing.
March 25, 2026 at 14:23
Katie Putbrese
This is why I hate modern medicine. They want to drug you up with letrozole and metformin like it’s a soda machine. Back in my day, women just ate real food, walked to the store, and had babies without all this tech. Now it’s all apps and blood panels and AI. Who even are these people running these trials? I’m not trusting some lab in Boston to fix my hormones.
March 27, 2026 at 08:18
Jacob Hessler
metformin gives me diareah and i hate it. why do docs keep pushing it? i just wanna get pregant not be sick all day. clomid worked fine for me. why complicate stuff?
March 28, 2026 at 05:10
Amber Gray
lmao they said 'lose weight' like it's easy 😂 i lost 30lbs and still no ovulation. now i'm on letrozole and it's working. but yea, they act like if you're not thin you're lazy. smh
March 30, 2026 at 05:12
Danielle Arnold
Wow. A 2000-word essay on PCOS that somehow still misses the point. The real issue? The medical industrial complex turning fertility into a subscription service. Next they’ll be selling AI ovulation predictions on Apple Watch.
March 31, 2026 at 11:48
Jesse Hall
I just want to say thank you for sharing this. My sister has PCOS and I never understood how deep it goes until now. I’m sharing this with her. She’s been feeling alone in this. You made her feel seen. ❤️
March 31, 2026 at 16:27
Donna Fogelsong
Insulin resistance? That’s just the tip. The real cause is glyphosate in our food supply and fluoridated water. Big Pharma doesn’t want you to know that. They profit off drugs not lifestyle. Read Dr. Mercola. The body heals when you remove toxins. Not when you take metformin.
April 1, 2026 at 12:20
Sean Bechtelheimer
the system is rigged. they made us eat corn syrup and then sold us drugs to fix it. 🤡 i know a guy who cured his PCOS with lemon water and fasting. no science needed. just vibes.
April 2, 2026 at 11:11
Seth Eugenne
For anyone feeling overwhelmed-this is doable. I started with 10 minutes of walking a day. Then added one veggie to dinner. Then cut soda. Slowly. No pressure. It’s not about perfection. It’s about showing up for yourself. You’re not behind. You’re healing.
April 3, 2026 at 10:35
rebecca klady
I’m 28, thin, and have PCOS. Everyone assumes I’m fine. I’m not. I’ve been trying for 2 years. No one talks about lean PCOS. Thanks for mentioning it. This helped.
April 4, 2026 at 22:27
Namrata Goyal
you think this is science? in india we just eat turmeric and yoga. no drugs. no apps. no american overcomplication. your body knows. you just need to stop listening to doctors.
April 6, 2026 at 04:19